




Gov. Rick Snyder has recommended creating a state health insurance “exchange,” and to promote the concept he's using the reassuring language of the comparatively modest version identified with the conservative Heritage Foundation. Gov. Snyder's administration, however, is steadily advancing toward creating a full blown state “Obamacare exchange,” which is not really an exchange as originally envisioned, but rather the agency through which the federal Patient Protection and Affordable Care Act will distribute its subsidies and impose its restrictions and mandates. (See below, “Health Insurance Exchanges: Heritage vs. Obamacare.”)
By the end of this month, the Synder administration plans to apply for a “Level 1” PPACA funding grant, which a Department of Community Health spokesperson said in an email “would be used toward further study and development of the exchange.” Crains reports the state also will apply for a PPACA Information Technology grant by year’s end, and quotes an official who says this requires enactment of legislation creating an exchange.
According to health care policy expert Ed Haislmaier of the Heritage Foundation, these grants come with strings attached that increasingly commit the state to creating an Obamacare exchange, not the far more limited entity his organization has promoted. He told Capitol Confidential this is why he recommends states refuse to take this money. (Two that did have since returned it — Kansas and Oklahoma.)
Many free market health policy experts who oppose the PPACA say refusing to create an exchange is one of the most important actions states can take to help bring down the federal health care law, while creating one helps entrench it. Some recent developments have strengthened the case for refusing, or at least waiting until 2013.
The federal law, however, creates a “prisoners dilemma” for governors and legislators: On the one hand, if a state does not create its own Obamacare exchange then the feds will set one up, and lawmakers fear this will mean a loss of state control. Gov. Snyder expressed this concern in his recent message on health care: “I do not support a ‘one size fits all’ federal approach to health reform, which is where we would be if we were to allow the federal government to run a health insurance exchange in Michigan.”
Case grows for “Just Say No”
But states may retain little if any meaningful “control” even if they do create their own exchanges, because these will have to comply with reams of ever-changing federal regulations, most of which have not even been written yet. The first of four initial installments was released in July; according to the Wall Street Journal: “The word ‘require’ appears 811 times in the 244-page rule and its 103-page supplement. ‘Must’ shows up 580 times — and this is merely HHS’s first batch of exchange mandates…”
In recent weeks the case for “Just Say No” has grown stronger as new flaws have been discovered in the language of the PPACA, possibly caused by the irregular manner in which it was rushed through Congress in March 2010. The first of these involves funding for the alternative federal exchanges: There is none. That is, the law fails to authorize an ongoing funding mechanism.
Officials at the federal Department of Health and Human Services believe they can shuffle other funds to cover the cost, at least for a while. But unless Congress corrects the deficiency — including a Republican House of Representatives that has already voted to repeal the PPACA — sustaining this on a permanent basis may become problematic.
More serious, the law fails to authorize payment through the federal exchanges of the individual insurance subsidies that are the heart of Obamacare. This flaw was discovered by David Hogberg of Investors Business Daily, who reported, “Yet Obamacare states that the tax credit is available to people who are enrolled in an ‘an exchange established by the state under (Section) 1311.’ It makes no mention of people enrolled in federal exchanges being eligible for the tax credit.” Note: The “tax credit” is actually a subsidy styled as a “credit.”
Resistance growing elsewhere, legislation introduced here
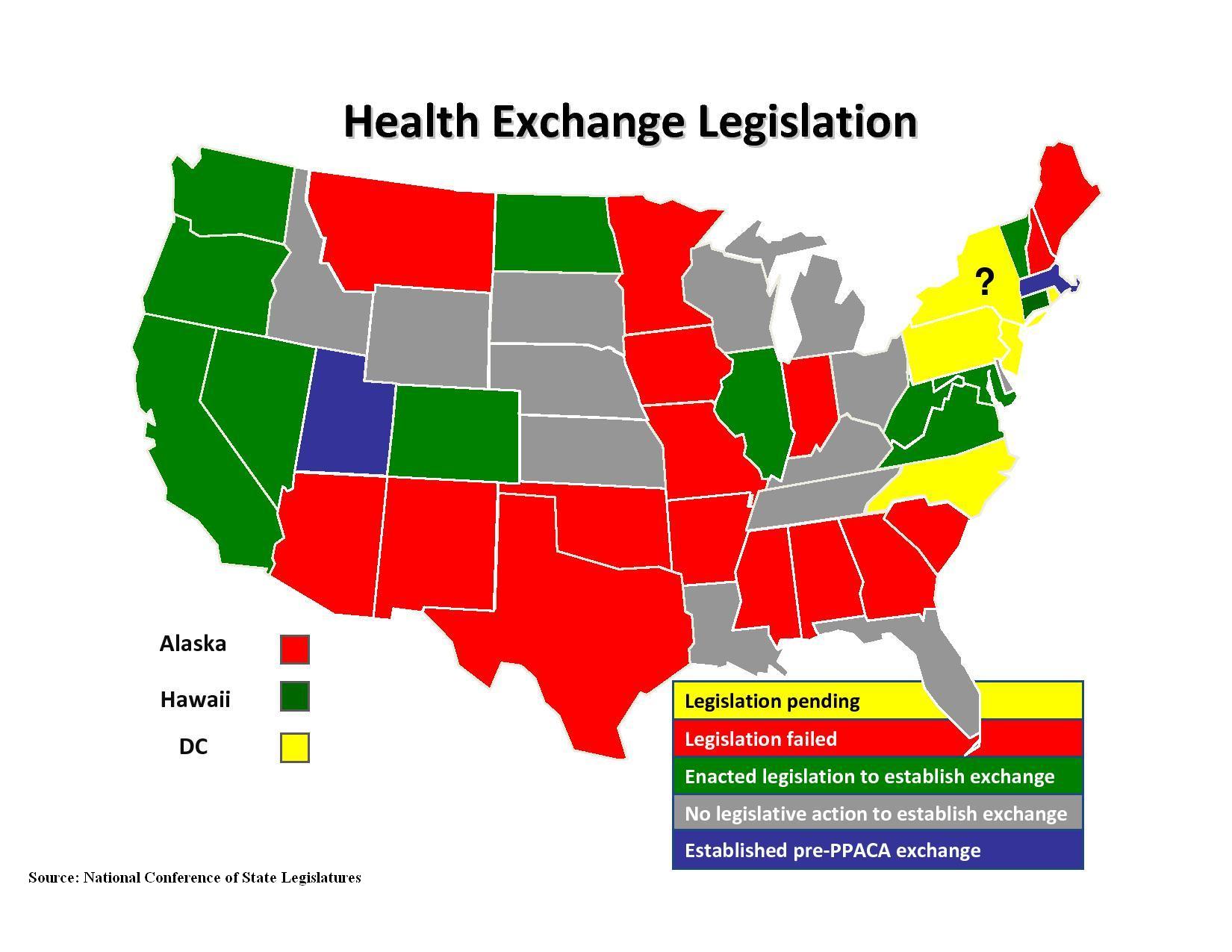
These flaws pose a serious challenge to the functioning of the law, especially if more than a handful of states fail or refuse to create an exchange. And resistance to doing so may be growing. At least five Republican governors have either flat-out refused, or have returned federal grants previously accepted for the purpose.* A number of state legislatures have defeated or refused to act on exchange legislation.
Earlier this month it was reported that the Republican-controlled New York state Senate was refusing to approve legislation necessary to meet a Sept. 30 deadline for a particular PPACA exchange grant. A political science professor there told the New York Times, “With a state as visible as New York, for the exchange to be obstructed is a very ominous sign for the ultimate implementation of the Affordable Care Act.”
"Ominous" because if more than a handful of states lack exchanges when Obamacare kicks-in in 2014, one plausible scenario is that the complex structure of the law could cause it to collapse of its own weight, even if PPACA survives potential court rulings.
All this forms the backdrop for consideration of exchange legislation introduced this month by three state Senate Republicans, including Senate Majority Leader Randy Richardville, R-Monroe. As introduced, the bill mostly just establishes the structure of a state exchange. It or the rulemaking authority it grants to state bureaucrats, however, could become the basis for something more like a detailed model appended to the final report of a “work group” convened by the state using a $1 million PPACA planning grant (full text here). The group consisted of several dozen individuals, primarily representatives of special interests who will financially benefit from an exchange (names and affiliations here, scroll to end).
Is Gov. Snyder's exchange an Obamacare "Trojan Horse?"
Notwithstanding Gov. Snyder’s assurance that his proposed exchange will simply “allow customers and small businesses to make more efficient and better informed decisions,” and that even without the PPACA, “I would still be in favor of utilizing technology to create a better customer service experience for Michiganders,” it seems clear that the calculus of Obamacare’s “prisoners dilemma” is what’s really driving action by politicians here, a conclusion reinforced by the pursuit of strings-attached federal grants.
An ungenerous interpretation is that the governor is deliberately using such language as a smokescreen for an Obamacare Trojan Horse. The tactic has been seen before. For example, a powerpoint created by the liberal-leaning Colorado Health Foundation in a presentation at the National Conference of State Legislatures used Heritage, Massachusetts and Utah exchanges to sell legislators on creating what inevitably will be Obamacare exchanges.
More likely is that the cautious Gov. Snyder genuinely believes that creating a state exchange along with some other measures could mitigate some of Obamacare's usurpations of state authority.
Gov. Snyder, however, may be mistaken when saying his creation will “both satisfy the requirements of the PPACA and improve the experience of purchasing health insurance coverage in Michigan." Health policy expert Michael Cannon of the Cato Institute, who believes that any kind of exchange is an expansion of big government whose bureaucracy will only grow, told Capitol Confidential in an email: "Studies of Wisconsin and Ohio show that Obamaare exchanges will increase health insurance premiums by 30 percent or more. Gov. Snyder is getting bad advice, in all likelihood from private insurance carriers that hope to profit from Obamacare's massive government subsidies."**
Gov. Snyder's style may be to avoid the high-wire brinksmanship of fellow GOP governors refusing to create an exchange, but policymakers here should also ask whether now is the time, rather than waiting until 2013 when the country knows better whether the PPACA will survive. Various Obamacare grant "deadlines" create a false sense of urgency, when in fact the current administration in Washington appears eager to hand out this money.
Michigan wouldn't be alone if it delayed. Health policy expert John Graham of the Pacific Research Institute wrote this week: "The likelihood of exchanges being up and running by January 2014 is vanishingly close to zero. Indeed, they may not exist at all except in very few states — whether or not President Obama wins re-election."
The Obama administration itself may recognize this, as shown by reports of a "new partnership model" that would, in the words of Department of Health and Human Services Regional Director Marguerite Salazar, "be the option for states that are nervous about a full-fledged exchange.”
Finally, it’s worth noting that the word “exchange” was rarely if ever mentioned during the various state political campaigns in 2010, including the Michigan Republican gubernatorial primary. Creating a state “exchange” has never been a priority on any Michigan politician's agenda, and there doesn't appear to be a home-grown demand for one (self-interested special interests aside).***
"Prisoners dilemmas" by their nature force unseemly choices. But Obamacare is not popular with the population in general, and is deeply unpopular among those who generally vote Republican. Politicians with “R” after their names should not be surprised if their constituents react very badly to all this. Or that if Obamacare survives to inflict its mandates and rationing of treatments that Michigan families need, future voters punish state politicians whose fingerprints are on it.
~~~~~~~~~~
Sidebar: Health Insurance Exchanges: Heritage vs. Obamacare
The exchange idea is one response to what many health policy experts view as the “original sin” that's caused most of the dysfunctions in our current health care system: The federal tax code allows employers to deduct the cost of health insurance fringe benefits for employees. This caused the gradual expansion of a “third party payer” system that wrecked the usual market incentives for consumers to be prudent, frugal value-seekers, which drives competing providers to be innovative, efficiency-generating value maximizers. Just one detail is relevant for the exchange issue, however: While employers can deduct employee health insurance costs, individuals who buy their own coverage must pay using after-tax dollars taken from their disposable income.
As originally conceived, state exchanges offer a two-fold response to this problem: They would allow individuals to purchase coverage with pre-tax dollars (that is, make the cost tax deductable), and allow employers (especially small businesses) to kick in part of the cost for employees who buy their own policy on the exchange. An additional benefit is that the coverage would be selected by and belong to the individual, not the employer. It would be “portable,” allowing a worker to take his or her coverage along when switching jobs.
The Heritage Foundation has been the leading proponent of the concept. Last year, the state of Utah launched a pilot program to create this kind of exchange, thus the terms “Heritage exchange” or “Utah exchange,” as opposed to a very different kind of entity, an “Obamacare exchange.” In fact, the latter is not really an exchange at all, as defined in the original concept. In a paper published earlier this year, Heritage Foundation health policy expert Ed Haislmaier explained the difference:
The first point to understand is that the entire design for health insurance exchanges in the PPACA is a perversion of the core concept of what is an otherwise sound approach to improving health insurance markets.
. . . Rather than serving as a mechanism for expanding health insurance choice, variety, and competition, and for spurring plans and providers to innovate and offer customers better value, Obamacare exchanges will impose new regulations, administer new subsidies, standardize coverage, and restrict consumer choice and insurer competition more than it is already. Thus, in the PPACA Congress has perverted the exchange concept into a bureaucratic tool for federal subsidization, standardization, and micromanagement of health insurance coverage by the Department of Health and Human Services.
Haislmaier and Heritage's support for non-Obamacare exchanges is not shared by most free-market health policy experts, who are skeptical about expansions of government intended to fix problems created by government. As the Cato Institute's health care expert Michael Cannon put it, "Fundamentally, there is no such thing as a market-friendly government bureaucracy."
Health policy expert John Graham of the Pacific Research Council wrote in a recent paper that the Utah exchange "almost certainly adds administrative costs to small businesses’ decisions to offer health benefits, without subtracting administrative costs from the old way of doing business.”
In addition, neither type of exchange is a government version of “Travelocity and Orbitz” for health insurance, as Gov. Snyder implied. If such a service is all he intends, the state can stand down, because the private sector already provides this — go to www.ehealthinsurance.com or www.getinsured.com to see examples. (I just told the latter my ZIP code, age and weight, and got dozens of quotes.)
~~~~~~~~~~
* Florida Gov. Rick Scott, Louisiana Gov. Bobby Jindal and Texas Gov. Rick Perry flat-out said "no" to creating exchanges. In addition, in August Kansas Gov. Sam Brownback ordered that $32 million in PPACA exchange grants be returned, and Oklahoma Gov. Mary Fallin returned $55 million in April.
** Cannon has described many more reasons legislators should be reluctant to create an exchange, as in this excerpt from testimony he gave to the Missouri Legislature: "You would be responsible for ensuring that carriers do not follow the law's enormous financial incentives to avoid, mistreat, and dump the sick. You would have to run a reinsurance program and a risk-adjustment program. You would have to define and monitor "network adequacy" as well as each insurance carrier's service area. You would have to monitor each carrier's marketing materials . . ."
*** Republican legislative health care reform packages were introduced in 2007 and 2009 containing an exchange, but appeared more to be “us too” statements responding to the initial enthusiasm generated by the adoption of “Romneycare” in Massachusetts than a home-grown demand for an exchange.
Michigan Capitol Confidential is the news source produced by the Mackinac Center for Public Policy. Michigan Capitol Confidential reports with a free-market news perspective.
 Whitmer has supported $16.2 billion in subsidies since 2001
Whitmer has supported $16.2 billion in subsidies since 2001
 Lawmakers a step closer to cutting income tax
Lawmakers a step closer to cutting income tax
 Michigan recycles economic development schemes
Michigan recycles economic development schemes